Incidence of Müllerian anomalies is up to 4% of reproductive age women. It occurs during fetal development and is already present at birth so it is a congenital disorder. During development of embryo, two paired Mullerian ducts turn into the female reproductive tract which includes, uterus, the fallopian tubes, cervix, and upper two thirds of the vagina.
The cause may be hereditary; random gene mutation or developmental defect.
Müllerian anomalies range from the absence of a uterus to the formation of a half uterus or a double uterus to a uterine division by a partition. All types of anomalies affect the reproductive outcome in varying degrees.
They include:
- Agenesis & hypoplasia: Mayer-Rokitansky-Kuster-Hauser syndrome is most common
- Unicornuate uterus: When one Mullerian duct fails to develop, a banana-shaped half-uterus is formed. Kidney problems accompany this asymmetric anomaly more than they do other Mullerian anomalies.
- Uterus didelphys: also called ‘double uterus’. Associated there may be complete duplication of the vagina, cervix and uterus, and the two halves may be divided by connective tissue. It has the best pregnancy outcomes amongst all anomalies.
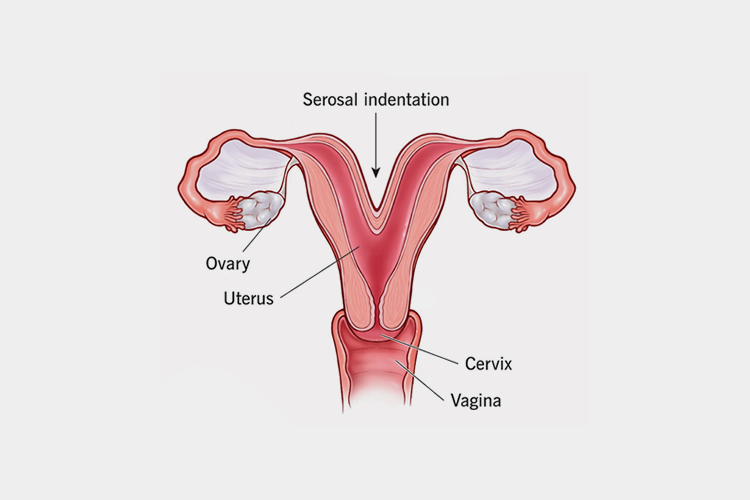
- Bicornuate uterus: This is the most common form of Mullerian anomaly. The womb is shaped like a heart, with a deep indentation at the top. This means that the baby has less space to grow than in a normally shaped womb.
- Septate uterus: when the cavity of the uterus is divided by a partition is called septum. The septum can be partial or complete
- Arcuate uterus: The fundus of the uterus is curved slightly both inside and outside. It is considered a variation of normal.
- DES-related uterus: A T-shaped uterine cavity, dilated uterine horns and malformed cervix and malformed upper vagina may characterize this anomaly. It happens due to ingestion of DES.
Müllerian anomalies are often diagnosed at the onset of puberty —when menstruation begins or when menstrual cycle fails to start. Few conditions may also be diagnosed when a woman has trouble in getting pregnant, or maintaining a pregnancy.
Three-dimensional pelvic ultrasound, laparoscopy hysteroscopy, MRI can diagnose a Mullerian anomaly and may also detect other existing Kidney defects. A combination of tests may be recommended to establish the most accurate diagnosis.
In many cases, the condition can be left untreated, if it does not affect fertility. Müllerian anomalies causing obstruction in menstruation or pain are usually treated by surgery.
Septate uterus (a partitioned uterus) can be corrected by hysteroscopy for improving chances of having a successful pregnancy.
For bicornuate uterus in limited cases laparoscopic Strassman metroplasty is performed.



